Quick Answer: What to Expect in the First 30 Days of Recovery?
- Days 1–7: Detox and acute withdrawal — often the hardest stretch physically.
- Days 8–14: Medical stabilization; brain chemistry begins to shift.
- Days 15–21: Therapy engagement begins; emotional turbulence peaks for many.
- Days 22–30: Routine builds; early coping skills form the foundation of lasting recovery.
- The goal: Survive the first week, stabilize the second, begin to heal in the third and fourth.
The first 30 days of recovery are simultaneously the most dangerous and the most transformative period a person in recovery will ever face. This is the window when withdrawal peaks, cravings hit hardest, and the brain begins — slowly, measurably — to rewire itself toward a life without substances.
This guide is not a motivational overview. It is a clinical, week-by-week account of what actually happens in the body and mind during early recovery: what to expect, what the research says, and what separates individuals who sustain sobriety from those who relapse before day 31.
Legal and Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Withdrawal from certain substances — including alcohol, benzodiazepines, and opioids — can be medically dangerous. Always consult a licensed medical professional before stopping or reducing substance use.
What Happens in the First 30 Days of Recovery?
The first 30 days of recovery involve four overlapping phases: acute detox and withdrawal (days 1–7), medical stabilization (days 8–14), initial therapy engagement (days 15–21), and early skill-building (days 22–30). During this period, the brain begins reversing the neurological damage caused by chronic substance use, though most cognitive and emotional functions do not fully normalize until 90 days or beyond.
Most people dramatically underestimate how much happens physiologically during this month. Withdrawal symptoms, sleep disruption, mood dysregulation, and intense cravings are not signs of weakness — they are the predictable, well-documented result of the brain and body recalibrating after chemical dependency.
Understanding the timeline removes the mystery. And removing the mystery is the first step toward surviving it.
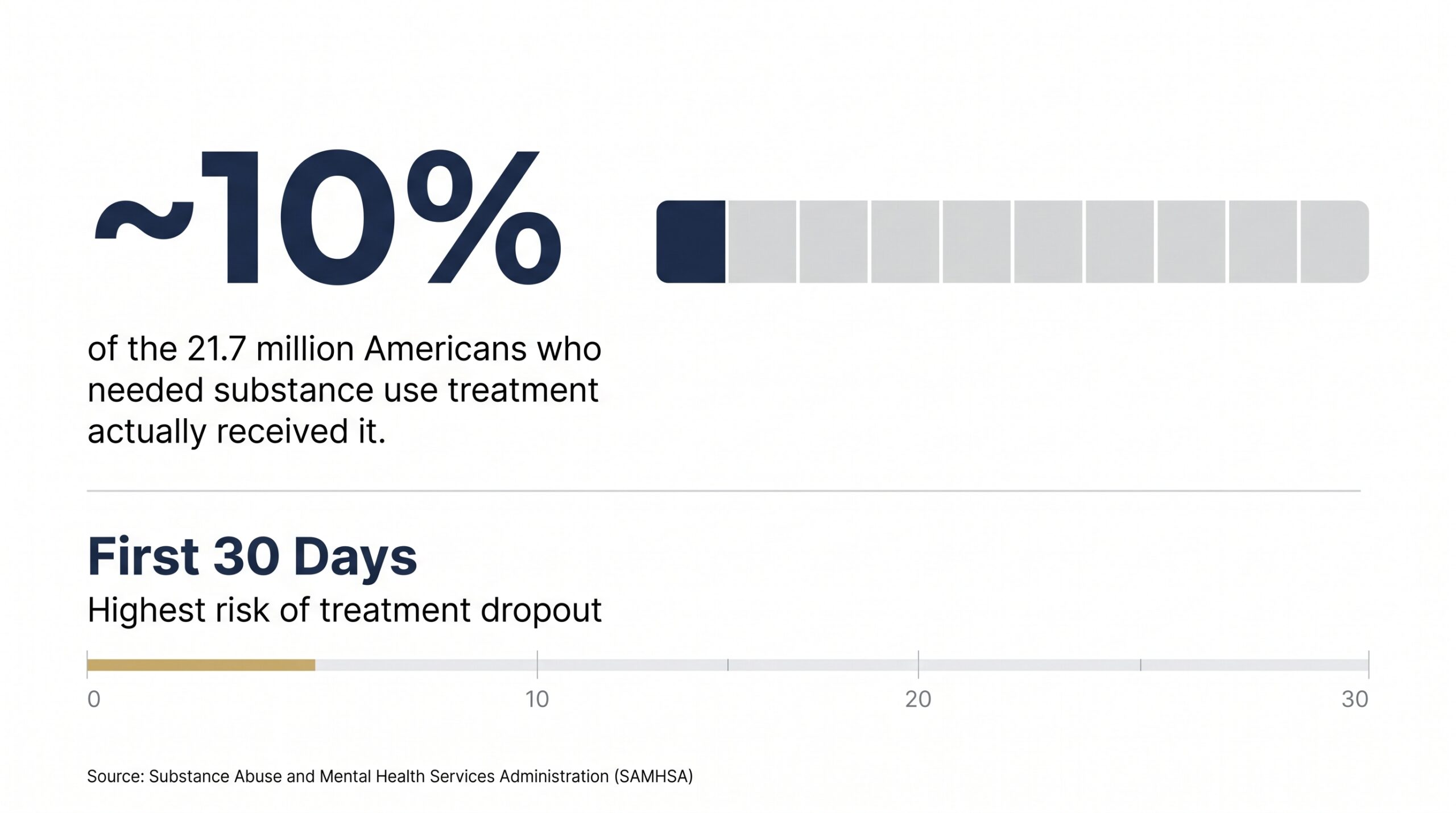
According to the Substance Abuse and Mental Health Services Administration (SAMHSA), only about 10% of the 21.7 million Americans who needed substance use treatment in a given year actually received it — and of those who do enter treatment, the first 30 days represent the period of highest dropout risk.
Source: SAMHSA
Days 1–7: Acute Detox and Withdrawal
During days 1 through 7 of recovery, the body undergoes acute withdrawal as it clears the substance and tries to restore neurochemical balance. This phase is the most physically intense stretch of early recovery. Symptoms vary significantly by substance but commonly include nausea, sweating, insomnia, anxiety, tremors, and intense cravings. For alcohol and benzodiazepine dependence, this phase can be life-threatening without medical supervision.
What Withdrawal Actually Feels Like — By Substance
Withdrawal is not a uniform experience. The specific symptoms, their severity, and their duration depend almost entirely on which substance was used, how long it was used, and the individual’s biology. Here is a clinical breakdown:
| Substance | Onset of Withdrawal | Peak Symptoms | Common Symptoms | Medical Risk Level |
|---|---|---|---|---|
| Alcohol | 6–24 hours after last drink | 24–72 hours | Tremors, sweating, seizures, delirium tremens (DTs) | HIGH — can be fatal |
| Opioids | 8–24 hours (short-acting); 36–48 hours (methadone) | Days 2–3 (short-acting); Days 3–5 (long-acting) | Muscle aches, vomiting, diarrhea, insomnia, anxiety, goosebumps | MODERATE — rarely fatal, but severe |
| Benzodiazepines | 1–4 days after last dose | Days 5–7 | Anxiety, seizures, psychosis, panic attacks | HIGH — can be fatal |
| Stimulants (meth, cocaine) | Hours after last use | Days 1–3 | Severe depression, fatigue, hypersomnia, intense cravings | LOW physical risk; HIGH psychiatric risk |
| Cannabis | 24–72 hours after last use | Days 2–6 | Irritability, insomnia, appetite loss, anxiety | LOW |
Note: This table represents typical ranges. Individual experiences vary widely. Always seek medical evaluation before beginning detox.
Why Medically Supervised Detox Matters
Attempting to detox from alcohol or benzodiazepines without medical supervision carries a documented risk of fatal seizures. Delirium tremens (DTs) — a severe form of alcohol withdrawal — occurs in an estimated 3–5% of people experiencing alcohol withdrawal and carries a mortality rate of up to 15% when untreated.
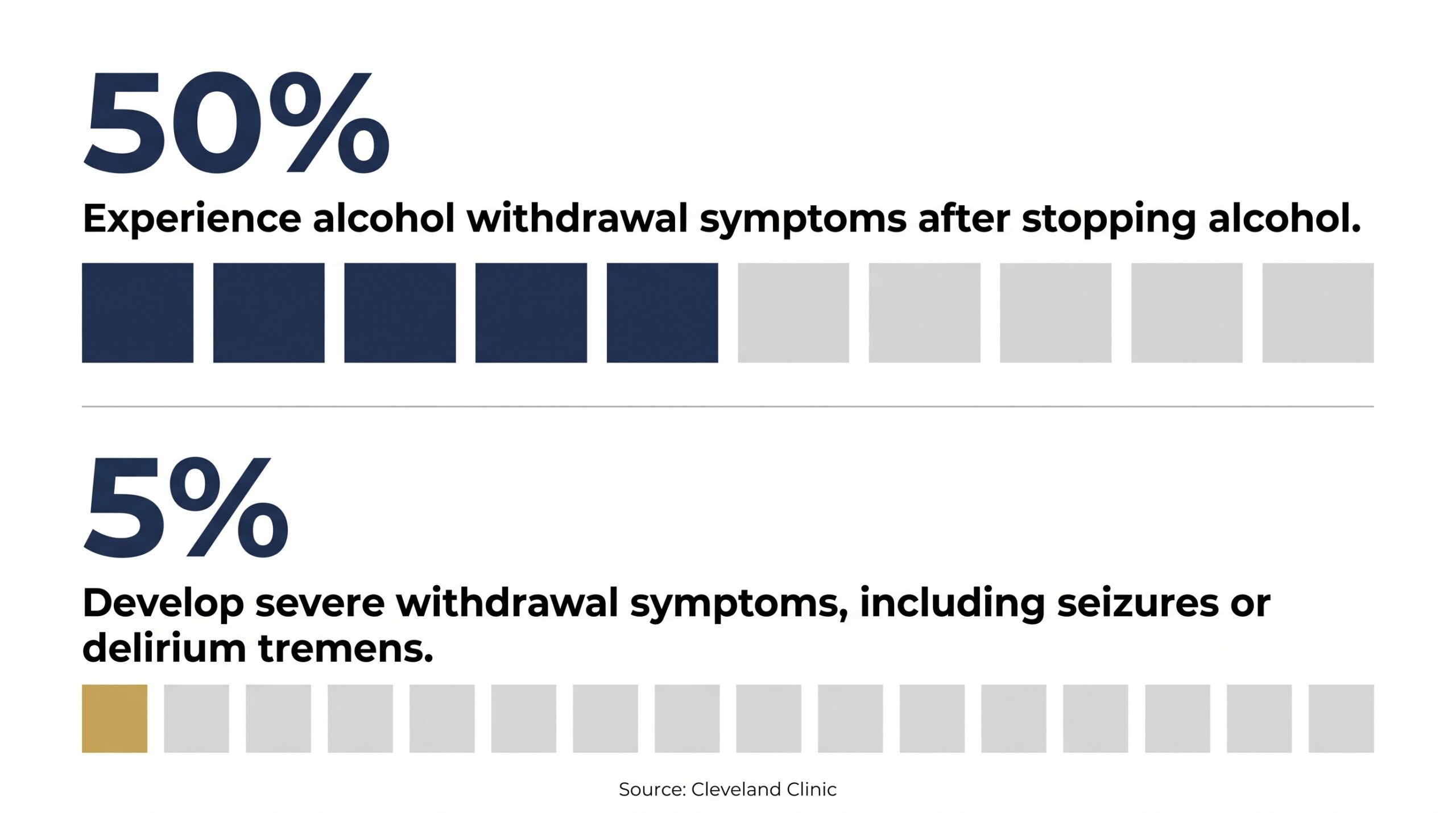
A clinical review published by Cleveland Clinic found that approximately 50% of individuals with alcohol use disorder will experience withdrawal symptoms upon cessation, and roughly 5% will develop severe withdrawal manifestations including seizures or delirium tremens.
Source: Cleveland Clinic
Medically supervised detox — available through inpatient programs, hospital settings, or clinical withdrawal management programs — uses medications like benzodiazepines (for alcohol), buprenorphine (for opioids), or clonidine (for multiple substances) to reduce withdrawal severity, prevent complications, and keep the person safe long enough to engage in actual treatment.
Days 8–14: Medical Stabilization and the Brain Begins to Shift
During days 8 through 14 of recovery, acute withdrawal typically subsides, but a subtler and longer-lasting phase begins: post-acute withdrawal syndrome (PAWS). The brain’s dopamine system — suppressed or dysregulated by chronic substance use — begins to recalibrate. Sleep remains disrupted. Mood swings are common. Cognitive fog lifts only slightly. However, the individual is now medically stable enough to begin engaging meaningfully in treatment.
Understanding PAWS: The Withdrawal Nobody Talks About
Post-Acute Withdrawal Syndrome is one of the most underrecognized phenomena in early recovery. While acute withdrawal (days 1–7) is dramatic and often what people prepare for, PAWS is quieter — and in many ways, more dangerous for long-term sobriety.
PAWS symptoms include:
- Persistent sleep disruption and insomnia
- Anhedonia — the inability to feel pleasure in previously enjoyable activities
- Difficulty with concentration and short-term memory
- Emotional blunting or mood swings that feel uncontrollable
- Variable but often intense cravings triggered by stress, boredom, or environmental cues
- Anxiety and low-grade depression, even in individuals with no prior mental health history
These are not psychological weaknesses. They are the measurable neurological consequences of the brain’s reward system attempting to restore baseline dopamine function after prolonged suppression or flooding.
Research published in the National Library of Medicine found that PAWS can persist for weeks to months following cessation of alcohol, opioids, and stimulants — and is a primary driver of relapse during early recovery, particularly in the absence of structured clinical support.
Source: NLM
What the Brain Is Actually Doing During Week Two
Chronic substance use alters the brain’s prefrontal cortex — the region governing decision-making, impulse control, and long-term planning — as well as the limbic system, which regulates emotion and motivation. During week two, these systems begin rebalancing, but the process is nonlinear and slow.
The practical implication: someone in week two of recovery may know intellectually that sobriety is the right choice, while simultaneously feeling emotionally incapable of imagining a life that feels good without the substance. This cognitive-emotional disconnect is normal, expected, and temporary. It is not a sign that treatment is failing.
Days 15–21: Therapy Engagement and Emotional Turbulence
During days 15 through 21, the individual is typically stable enough to engage meaningfully in individual therapy, group counseling, and structured treatment programming. This is also when the emotional reality of sobriety — grief, shame, trauma, and anxiety about the future — often surfaces for the first time without the buffer of substances. This phase is emotionally the most turbulent stretch of the first 30 days.
Why Feelings Get Worse Before They Get Better
One of the most important things clinicians tell clients entering their third week of recovery is this: “You may feel worse this week than you did in week two. That is expected. That is progress.”
Substances function, among other things, as emotional anesthetics. When someone drinks or uses to cope with anxiety, trauma, grief, or boredom, those underlying emotional states do not disappear — they are suppressed. In week three, without chemical suppression, those emotions emerge. Sometimes all at once.
This emotional surfacing is not a crisis. It is the beginning of real work. But without clinical support to name, process, and contextualize these feelings, it is also one of the most common triggers for early relapse.

SAMHSA reports that approximately 21.2 to 21.5 million adults in the U.S. have co-occurring mental health and substance use disorders. Among individuals in early recovery, unaddressed anxiety and depression are among the leading predictors of relapse in the first 30 days.
Source: SAMHSA
Evidence-Based Therapies That Begin in Week Three
Quality treatment programs introduce structured, evidence-based therapies during this window. The most widely validated modalities for early recovery include:
- Cognitive Behavioral Therapy (CBT): Identifies the thought patterns that trigger cravings and teaches concrete interruption strategies. CBT is among the most researched interventions in addiction treatment and has demonstrated effectiveness across alcohol, opioid, stimulant, and cannabis use disorders.
- Motivational Interviewing (MI): A clinician-guided conversation style that helps individuals articulate their own reasons for change. MI is particularly effective in early recovery when ambivalence about sobriety is still high.
- Dialectical Behavior Therapy (DBT) skills: Distress tolerance, emotional regulation, and interpersonal effectiveness skills — the exact competencies most challenged in early recovery.
- Trauma-informed care: Because unresolved trauma underlies a significant percentage of substance use disorders, trauma-sensitive therapy modalities are increasingly integrated into first-30-day programming.
- Group therapy: Peer support in a structured clinical setting reduces isolation — one of the most dangerous emotional states in early recovery — and provides real-time modeling of coping strategies by people slightly further along in the process.
The Role of Medication-Assisted Treatment (MAT)
By week three, individuals with opioid or alcohol use disorder who are appropriate candidates for Medication-Assisted Treatment (MAT) are typically stabilized on FDA-approved medications — buprenorphine/naloxone (Suboxone), naltrexone (Vivitrol), or acamprosate. The evidence base for MAT is unambiguous.
The National Institute on Drug Abuse (NIDA) states that medications for opioid use disorder (MOUD), including buprenorphine and methadone, drastically reduce illicit opioid use, lower overdose mortality, decrease criminal justice involvement, and increase patient retention in treatment. While counseling and behavioral therapies are highly valuable components that address the psychological aspects of recovery, clinical data shows that MOUD is profoundly effective on its own and should never be withheld if behavioral services are unavailable or declined by the patient.
Source: NIDA
Days 22–30: Building Routine, Skills, and a Recovery Identity
During days 22 through 30, the acute biological crisis of early recovery has passed. The central task of this phase is building structure: daily routines, coping skill practice, peer connections, and the beginning of an identity as someone in recovery — not just someone who stopped using. This is the week when treatment starts to feel less like survival and more like the first chapter of a different life.
Why Routine Is a Clinical Tool, Not Just Good Advice
Structure is not a lifestyle preference in early recovery — it is a neurological intervention. The brain in early recovery has a weakened capacity for executive function: planning, impulse control, and managing ambiguity. Predictable routines reduce the cognitive load on a prefrontal cortex that is still healing.
Effective treatment programs in this phase help clients build:
- Consistent sleep and wake schedules (sleep dysregulation remains a primary relapse risk in week four)
- Regular meal timing to stabilize blood sugar, which significantly affects mood and craving intensity
- Daily scheduled therapy, group sessions, and peer check-ins
- Physical activity — even mild exercise has documented effects on dopamine regulation and mood in early recovery
- A concrete plan for high-risk times: evenings, weekends, and situations previously associated with use
A study published in Mental Health and Physical Activity found that even moderate aerobic exercise (30 minutes, 3x per week) significantly reduced cravings and improved mood in individuals with substance use disorders during early recovery. Exercise’s effect on dopamine and serotonin systems partially compensates for the neurochemical deficits of early abstinence.
Source: Science Direct
Peer Support and the Power of Shared Experience
By day 22, most individuals in structured treatment have begun forming genuine connections with peers in their treatment cohort. This is not incidental — it is one of the most clinically significant things that happens in the first 30 days.
Social isolation is among the strongest predictors of relapse. Peer connection — especially with others who have experienced addiction firsthand — provides validation that no clinician can fully replicate. Twelve-Step programs, SMART Recovery, and peer support specialists are typically introduced and integrated during this phase.
Planning for What Comes After Day 30
A 30-day program is a beginning, not a conclusion. The most important conversation that happens at day 30 is the one about what comes next.
NIDA’s research is explicit: most individuals with substance use disorder need at least 90 days of treatment to significantly reduce or stop drug use, and that better outcomes are consistently associated with longer durations of care and structured step-down support.
The standard step-down continuum following a 30-day residential or intensive program is:
- Partial Hospitalization Program (PHP): 5–6 hours of structured programming per day, 5 days per week. Allows the individual to sleep at home or in sober living while maintaining intensive clinical contact.
- Intensive Outpatient Program (IOP): 9–12 hours per week of group and individual therapy. The bridge between full immersion and independent living.
- Standard Outpatient: Weekly or biweekly individual therapy sessions and ongoing psychiatric/MAT management as needed.
- Peer support and community: Ongoing 12-Step, SMART Recovery, or other peer-based support structures maintained throughout all levels of care.
Research found that individuals who completed a full continuum of care — from residential treatment through outpatient — had significantly better 12-month sobriety outcomes than those who received only a single level of care. Continuity, not intensity alone, drives long-term outcomes.
Sources: NLM, American Family Physician
Physical Changes You Can Expect in the First 30 Days
During the first 30 days of recovery, the body undergoes measurable physical restoration. Liver enzyme levels begin to normalize within 2–4 weeks of alcohol cessation. Skin quality improves as hydration is restored. Cardiovascular function begins to recover. Sleep — while severely disrupted in weeks one and two — gradually improves by weeks three and four for most individuals. These changes are real, measurable, and accelerating.
A timeline of common physical changes:
- Days 1–3: Dehydration, nausea, sweating, appetite disruption
- Days 4–7: Appetite begins to return; initial energy improvement possible; sleep still disrupted
- Days 8–14: Liver begins recovering; skin hydration improves; blood pressure often reduces in alcohol-dependent individuals
- Days 15–21: Energy more consistent; GI function stabilizes; weight may begin shifting (gain or loss depending on substance and nutrition history)
- Days 22–30: Noticeable improvement in skin clarity, energy, and physical stamina; cognitive fog lifting; sleep quality improving
According to research, liver fat content measurably decreases within 2–6 weeks of alcohol abstinence in individuals with alcohol-related fatty liver disease, and liver enzyme markers (ALT, AST) begin normalizing within 4 weeks for most patients who stop drinking.
Sources: NLM, Recovered, Sip Yours
What the Research Says About Relapse Risk in the First 30 Days
The first 30 days of recovery carry the highest relapse risk of any period in the recovery process. Studies consistently show that 40–60% of individuals with substance use disorders relapse within the first year, with the highest concentration of those relapses occurring in the initial weeks. Understanding the specific triggers — rather than treating relapse as moral failure — is what allows clinicians and families to intervene effectively.
The most evidence-supported relapse triggers in the first 30 days:
- Environmental cues: People, places, and objects associated with prior use trigger conditioned cravings that can feel physically overwhelming
- Untreated co-occurring disorders: Depression, anxiety, PTSD, and ADHD that were previously self-medicated resurface acutely in early abstinence
- Social isolation: The absence of peer connection and meaningful structure is one of the most reliable predictors of relapse
- Overconfidence after acute withdrawal: Feeling better after week one sometimes creates a false sense that the hard work is done
- HALT states: Being Hungry, Angry, Lonely, or Tired dramatically lowers resistance to cravings — basic self-care is a clinical intervention
NIDA notes that relapse rates for substance use disorders range from 40 to 60 percent — comparable to other chronic medical conditions such as hypertension and asthma. This framing is not to normalize relapse but to underscore that it is a clinical event requiring treatment adjustment, not evidence that recovery is impossible.
Source: NIDA
A note from our clinical team at Ridgeline Recovery: the clients we have seen complete the first 30 days of recovery most successfully are not those who suffered least. They are those who were most honest about what they were feeling, most willing to ask for help during hard moments, and most consistent in showing up — not because they felt like it, but because they had made a decision.
How Families Can Support Someone in Their First 30 Days
Family members play a measurable role in early recovery outcomes. Research consistently shows that social support — particularly from family — is among the strongest predictors of treatment retention and long-term sobriety. However, the nature of that support matters. Enabling behaviors, high-conflict communication, and enmeshed boundaries consistently undermine recovery, even when motivated by love.
Evidence-based ways families can help during the first 30 days:
- Remove access to substances from the home. This includes alcohol, prescription medications not prescribed to the individual in recovery, and paraphernalia.
- Participate in family therapy when offered. Treatment programs that include family therapy components have documented better retention and outcome rates than those that address only the individual.
- Learn the CRAFT model. Community Reinforcement and Family Training is an evidence-based approach that teaches family members how to support recovery through positive reinforcement and healthy boundary-setting — without ultimatums or confrontation.
- Expect emotional volatility. Mood swings in weeks two and three are neurologically driven, not directed at you. Clinical preparation for this reality protects family relationships through one of the hardest phases.
- Take care of yourself. Secondary trauma, burnout, and enabling are nearly universal in families affected by addiction. Al-Anon, Nar-Anon, and therapist-guided family support are not optional extras — they are part of the treatment system.
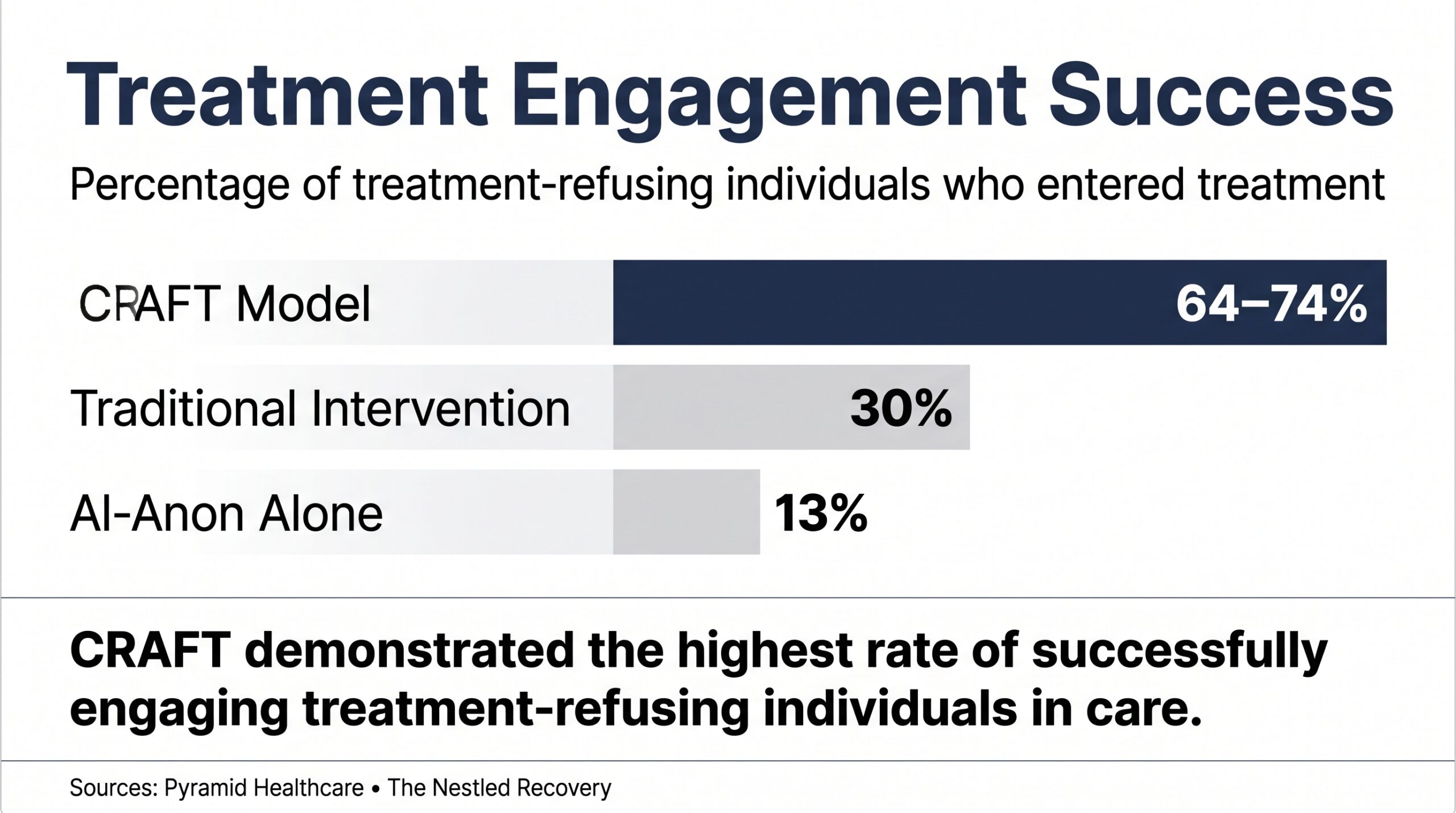
A randomized controlled trial found that the CRAFT model was effective in engaging treatment-refusing individuals in treatment in 64–74% of cases — significantly outperforming Al-Anon alone (13%) and traditional intervention (30%) in getting loved ones to enter treatment.
Sources: Pyramid Healthcare, The Nestled Recovery
Ridgeline Recovery: Supporting Your First 30 Days and Beyond
At Ridgeline Recovery in Columbus, Ohio, we provide comprehensive, evidence-based treatment across every level of the care continuum — from initial clinical assessment through Partial Hospitalization, Intensive Outpatient, and long-term aftercare. We accept most major insurance plans, including Ohio Medicaid.
If you or someone you love is approaching the first 30 days of recovery, our clinical team is ready to walk through every phase of the process with you — from detox coordination and medical stabilization through therapy, peer support, and step-down planning.
Frequently Asked Questions
What is the hardest part of the first 30 days of recovery?
For most people, the hardest part is not the first week — it is the transition into weeks two and three, when the acute physical crisis has passed but the emotional reality of sobriety fully arrives. Post-acute withdrawal symptoms, unaddressed co-occurring mental health conditions, and the grief of leaving behind a substance that functioned as a coping mechanism all converge in this window. Structured clinical support during this period is not optional — it is what statistically separates sustained recovery from early relapse.
Can you detox at home in the first 30 days of recovery?
Detox from alcohol and benzodiazepines at home is medically dangerous and can be fatal. Delirium tremens and withdrawal seizures require medical supervision and medication management. Opioid withdrawal is rarely fatal but is severe enough that unsupervised detox dramatically increases the risk of relapse and overdose due to reduced tolerance. Medically supervised detox is the clinical standard for any moderate-to-severe substance use disorder.
How long do cravings last in early recovery?
Acute cravings — the intense, sudden urge to use — typically peak in the first two weeks and decrease in frequency and intensity over the following months. However, cue-triggered cravings (triggered by people, places, or emotions associated with prior use) can persist for months to years and are a primary driver of long-term relapse. Behavioral therapies like CBT and mindfulness-based relapse prevention specifically target cue reactivity and are most effective when started within the first 30 days.
What should you eat during the first 30 days of recovery?
Nutrition is an underutilized clinical tool in early recovery. Chronic substance use commonly causes significant nutritional deficiencies — particularly B vitamins (especially thiamine in alcohol use disorder), zinc, magnesium, and protein. A 2025 systematic review in Nutrients found that malnutrition and micronutrient deficiency are prevalent across all major substance use disorders and are most clinically acute immediately after detoxification, when deficiencies are no longer masked by the substance. A diet emphasizing whole proteins, complex carbohydrates, healthy fats, and micronutrient-rich foods supports neurological repair, mood stabilization, and energy regulation. Many evidence-based treatment programs now integrate nutritional assessment and counseling as a standard component of first-30-days care.
Is 30 days of treatment enough to get sober?
Thirty days is enough to survive detox, stabilize medically, begin therapy, and build an initial foundation. It is not enough to complete recovery. NIDA’s clinical guidelines state that most individuals need a minimum of 90 days of treatment to significantly reduce or stop drug use, with better outcomes consistently associated with longer durations and structured step-down programming. A 30-day program is the starting line, not the finish line.
What happens to the brain during the first 30 days of sobriety?
During the first 30 days without substances, the brain begins reversing some of the structural and functional changes caused by chronic use. Dopamine receptors that were downregulated by prolonged substance exposure begin to upregulate. The prefrontal cortex — the region governing impulse control and decision-making — shows early signs of functional recovery. However, neurological restoration is a slow process: full cognitive recovery from heavy substance use often takes 6–12 months or longer, which is why the work of recovery must extend well beyond day 30.
What is the difference between detox and treatment in the first 30 days?
Detox is the process of safely clearing the substance from the body and managing withdrawal symptoms. It is medically necessary but not sufficient. Treatment — which begins after or during detox — addresses the psychological, behavioral, and social dimensions of addiction through therapy, counseling, peer support, and skill-building. Many families and individuals make the mistake of believing detox alone constitutes treatment. It does not. Detox without subsequent treatment has extremely high relapse rates.
What are the signs that someone is doing well in their first 30 days of recovery?
Positive indicators in early recovery include consistent attendance at treatment sessions, willingness to discuss difficult emotions rather than suppress them, beginning to form connections with peers in recovery, demonstrating awareness of personal triggers, and engaging in basic self-care including sleep, nutrition, and exercise. Progress in early recovery is rarely linear — it often looks like two steps forward and one step back. The relevant measure is directional trend, not day-to-day performance.
Sources & References
-
Able 2 Change Recovery. (2026). Pink clouding: Understanding the early stages of recovery. Able 2 Change Recovery. https://able2changerecovery.com/pink-clouding/
-
American Academy of Family Physicians. (1998, July 1). Outpatient management of alcohol withdrawal syndrome. American Family Physician, 58(1), 139–146. https://www.aafp.org/afp/1998/0701/p139.html
-
Cleveland Clinic. (2025, April 14). Alcohol withdrawal: Symptoms, causes, and treatment. Cleveland Clinic Health Library. https://my.clevelandclinic.org/health/diseases/alcohol-withdrawal
-
National Institutes of Health. (2014). The neurobiology of substance use disorders (PMC4007701). National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC4007701/
-
National Institutes of Health. (2015). Neurocircuitry of addiction (PMC4553654). National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553654/
-
National Institutes of Health. (2016). Facing addiction in America: The Surgeon General’s report on alcohol, drugs, and health (Report No. NBK424859). U.S. Department of Health and Human Services. https://www.ncbi.nlm.nih.gov/books/NBK424859/
-
National Institutes of Health. (2017). Molecular mechanisms of drug addiction (PMC5513682). National Center for Biotechnology Information. https://pmc.ncbi.nlm.nih.gov/articles/PMC5513682/
-
Pyramid Healthcare. (2021, March 10). What should I know about the CRAFT intervention model? Pyramid Healthcare Blog. https://www.pyramid-healthcare.com/blog/2021/03/10/what-should-i-know-about-the-craft-intervention-model/
-
Recovered. (2026). Health benefits when you stop drinking alcohol. Recovered.org. https://recovered.org/alcohol/benefits-when-you-stop-drinking-alcohol
-
ScienceDirect. (2011). Neurobiological mechanisms of addiction and active recovery. Journal of Substance Abuse Treatment, 41(2), 115–124. https://www.sciencedirect.com/science/article/abs/pii/S1755296611000317
-
Sip Yours. (2026). Alcohol and liver health: What happens when you stop drinking. Sip Yours News. https://sipyours.com/blogs/news/alcohol-and-liver-health
-
Substance Abuse and Mental Health Services Administration. (2024, November 19). Release of the 2024 NSDUH: Leveraging the latest substance use and mental health data. U.S. Department of Health and Human Services. https://www.samhsa.gov/blog/release-2024-nsduh-leveraging-latest-substance-use-mental-health-data-make-america-healthy-again
-
Substance Abuse and Mental Health Services Administration. (2026). Trends in substance use admissions (SAMHSA Short Report No. 2716). Center for Behavioral Health Statistics and Quality. https://www.samhsa.gov/data/sites/default/files/report_2716/ShortReport-2716.html
-
The Nestled Recovery. (2025, August 4). How to convince someone to go to rehab. The Nestled Recovery Boutique Rehab Blog. https://thenestledrecovery.com/rehab-blog/how-to-convince-someone-to-go-to-rehab/
-
U.S. National Institute on Drug Abuse. (2020). Drugs, brains, and behavior: The science of addiction [PDF file]. National Institutes of Health. https://sbmi.uth.edu/heroes/documents/Science-of-Addiction-NIDA.pdf
-
U.S. National Institute on Drug Abuse. (2026a). Drug misuse and addiction. National Institutes of Health Series. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/drug-misuse-addiction
-
U.S. National Institute on Drug Abuse. (2026b). Medications for opioid use disorder. National Institutes of Health Research Topics. https://nida.nih.gov/research-topics/medications-opioid-use-disorder